
Introduction
Asthma is an intermittent reversible obstructive airway disease characterized by episodic narrowing of the airways and increased viscid mucus secretions causing dyspnoea. Asthma is a Greek work meaning panting.
Asthma is a paroxysmal dyspnoea accompanied by adventitious sound caused by a spasm of bronchial tubes or due to swelling of their mucus membranes.
 |
| Photo by CHEST Foundation - American College of Chest Physicians |
BRONCHIAL ASTHMA
In bronchial asthma, it should be noted that it is;
- It is a chronic disease.
- It is reversible.
- It is characterized by acute attack.
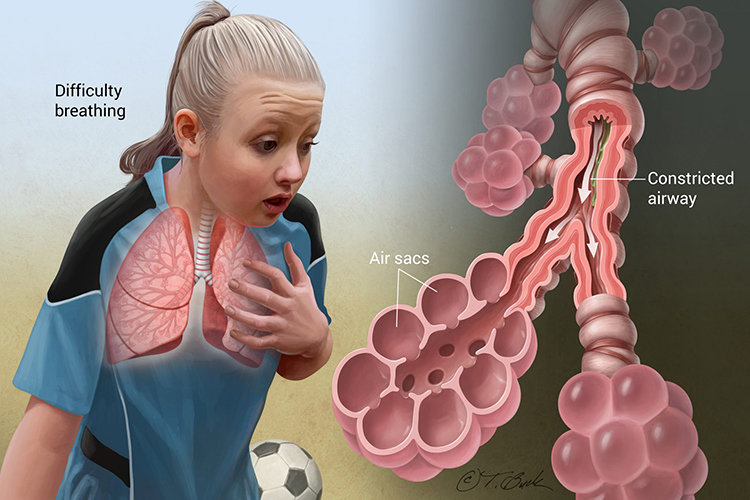
- It is characterized by difficulty in breathing.
- It is associated with wheezy respiration.
- Incidence/prevalence.
Asthma is considered to have a hereditary predisposition and has established global prevalence, of up to 5-20 years.
Risk Factors
The underlying mechanisms responsible for attacks of paroxysmal wheezing and dyspnoea are not known, but the following are the associated factors;
- Viral respiratory infections (common cold).
- Excessive anxiety or stress (emotional upset)
- Cold weather
- Certain foods (e.g. chocolate)
- Other infections (e.g. bronchitis) this could be either viral or bacterial
- Allergens, for example, dust, animal hairs etc.
- Drugs- beta blockers and aspirin.
- Environmental contaminants e.g. air pollution
- Climatic (weather) change
- Occupational exposures e.g. saw dust, fresh paint
- Stress-emotional upset and anxiety
Types of Bronchial Asthma
There are basically two types of bronchial asthma.
Extrinsic bronchial asthma
This occurs in children and younger age group who have hypersensitivity to foreign substances (risk factors). A history of infantile, eczema, high fever and urticaria as food allergens are common. The attack in this type are always gradual and eventually become frequent and having longer durations. It is believed to be hereditary.
Intrinsic bronchial asthma
This occurs in adults and there is no history of childhood allergy. It is associated with chronic inflammation of the upper respiratory tract. Emotional stress, extreme exercise, anger and anxiety are also contributing factors.
Pathophysiology
Asthmatic attacks are characterized by narrowing of the large and small airway tubes due to bronchial smooth muscle spasm, oedema and inflammation in bronchial mucosal wall and tenacious mucus secretions resulting in decreased alveolar ventilation. Continued under ventilated areas of the lungs leads to a ventilation imbalance resulting in hypoxaemia. Hyperventilation occurs as a result of partial pressure of carbon dioxide in blood (PaCO2)which further progress and worsens the attack.
Investigations
- Arterial blood gas analysis.
- Clinical findings.
- Personal or family allergic history.
- Chest x-ray.
- Pulmonary function test.
Clinical Features
SUBJECTIVE
- Rapid breathing
- Extreme fatigue
- Abdominal pain
- Occasional vomiting
- Tightness of the chest
OBJECTIVE
- Tachycardia
- Nasal flaring
- Wheezing and prolong expiration
- Diaphoresis
- Use of accessory muscle for breathing
- Occasional cyanosis
- Confusion
- Dyspnoea
- Dehydration
Medical Management
There are four classes of drugs that are mostly used
- The B-adrenergic agents- these cause bronchial smooth muscle relaxation e.g. epinephrine, salbutamol.
- Theophyline and its derivatives e.g Aminophyline. These also cause bronchial smooth muscle relaxation.
- Corticosteroids: This reduces oedema and inflammation of the bronchial tubes e.g. hydrocortisone.
- Cromolyn sodium: this represents a new class of agents which appear to directly inhibit mediator release independently. It interferes with calcium transport across cell membranes which may occur for its beneficial effects.
Nursing Management
- Monitor vital signs especially respiration.
- Nurse patient in a sitting position.
- Observe skin for colour and diaphoresis.
- Give humidified oxygen.
- Administer prescribed medication.
- Monitor input/output charts.
- Encourage plenty fluid intake.
- Reassure to reduce anxiety.
- Teach patient/family about condition (causes/prevention).
- Ensure enough ventilation.
- Improve diet.
- Encourage and provide rest.
Complications
- Lobar pneumonia
- Bronchopneumonia
- Corpulmonale
- Spontaneous pneumothorax
- Emphysema
- Bronchitis
- Atelectesis
- Broncheictasis
CARDIAC ASTHMA
This develops when fluids collects in the lungs due to heart failure. It is a paroxysmal nocturnal dyspnoea often accompanied by wheezing and coughing and may not be relieved by sitting up. An acute pulmonary oedema may occur particularly when there is a high workload on a damaged left ventricle (left ventricular failure).
It is a state of acute pulmonary congestion with hyperventilation and obstruction of the air way passages.
Status Asthmaticus
This describes an attack of asthma where one (initial) attack runs into the next attack without the patient getting relief in between the attacks.
The first sign of this attack is that the patient is unable to get relief from the usual medications. The common signs are exhaustive, acidosis, cyanosis, anoxia, tachycardia and monosyllabic speech.
It is a medical emergency and needs immediate hospitalization.
Managememnt
- Administer prescribed drugs.
- Relaxation is key and must be achieved by any means available.
- Nurse patient in a sitting position.
- Administer oxygen.
- Reassure the patient.
- Suction secretions..
Read Also






0 Comments