
Introduction
More commonly, diarrhea is a clinical syndrome in which there is frequent passage or unusually loose or watery bowel stool usually three or more in a 24hrs period sometimes accompanied by vomiting and fever, abdominal pain or cramps, fecal urgency, tenesmus, or the passage of bloody or mucoid stools. Diarrhea is usually caused by infection (especially in childhood); however, various disorders may cause this condition including malabsorption Syndromes and other intestinal abnormalities.
- Increased frequency of bowel movements (more than three per day).
- Increased amount of stool (more than 200g per day for the teenager and young adult or 10mL/kg/day for the infant and young child).
- Altered consistency (i.e. looseness) of stool.
- Diarrhea episodes are classically distinguished into acute and chronic (or persistent based on their duration).
Acute diarrhea is thus defined as an episode that has an acute onset and lasts no longer than 14 days.
Chronic or persistent diarrhea is defined as an episode that lasts longer than 14days.
Acute onset diarrhea is usually self-limited; however an acute infection can have a protracted course. By far, most common complication of acute diarrhea is dehydration.
Aetiology
- Infections e.g. bacteria, viruses, protozoa, fungi.
- Drugs e.g. antibiotics, laxatives, antacids that contain magnesium.
- Food allergies and intolerances e.g. cow’s milk protein allergy.
- Chemotherapy or exposure to radiation.
- Condition of the colon.
- Nutritional deficiencies and toxicity e.g. niacin deficiency/toxicity, kwashiorkor.
- Ingestion of heavy metals e.g. copper, zinc.
- Ingestion of certain poisonous plants e.g. amanita sp. of mushrooms.
- Other illness or disease e.g. HIV, DM
Risk Factors
- Failure to exclusively breastfeed infants.
- Use of infant breastfeeding bottles.
- Early termination of breastfeeding (before 1 year).
- Storing cooked food at room temperature.
- Poor personal and environmental hygiene e.g. inadequate hand hygiene practices, poor waste disposal.
- Malnutrition
- Immunosuppression
Mode of transmission
Infectious diarrhea is spread by the faecal-oral route. The most common sources are;
- Contaminated food and water.
- Person-to-person contact.
- Direct contact with infected faeces.
Classification
There are 3 broad classification of diarrhea.
Non-inflammatory diarrhea
This type of diarrhea is characterized by a watery, non-bloody bowel movement that is associated with diffuse abdominal cramping, nausea, vomiting or bloating.
- Typically mild but may be voluminous, involving large amounts of fluid (10- 20mL/kg/day).
- Fluids loss results in dehydration and loss of electrolytes. There is usually no blood loss.
- Common cause is a toxin producing organism e.g. Escherichia coli, staphyiococcus aureus
Inflammatory diarrhea
This type of diarrhea is characterized by the presence of fever and blood in the stool and is associated with left lower quadrant cramps, urgency and tenesmus (anal spasms).
- Fluid loss is minimal (less voluminous, less than 1 liter per day).
- Common cause; Camphylobacter or Yersinia species.
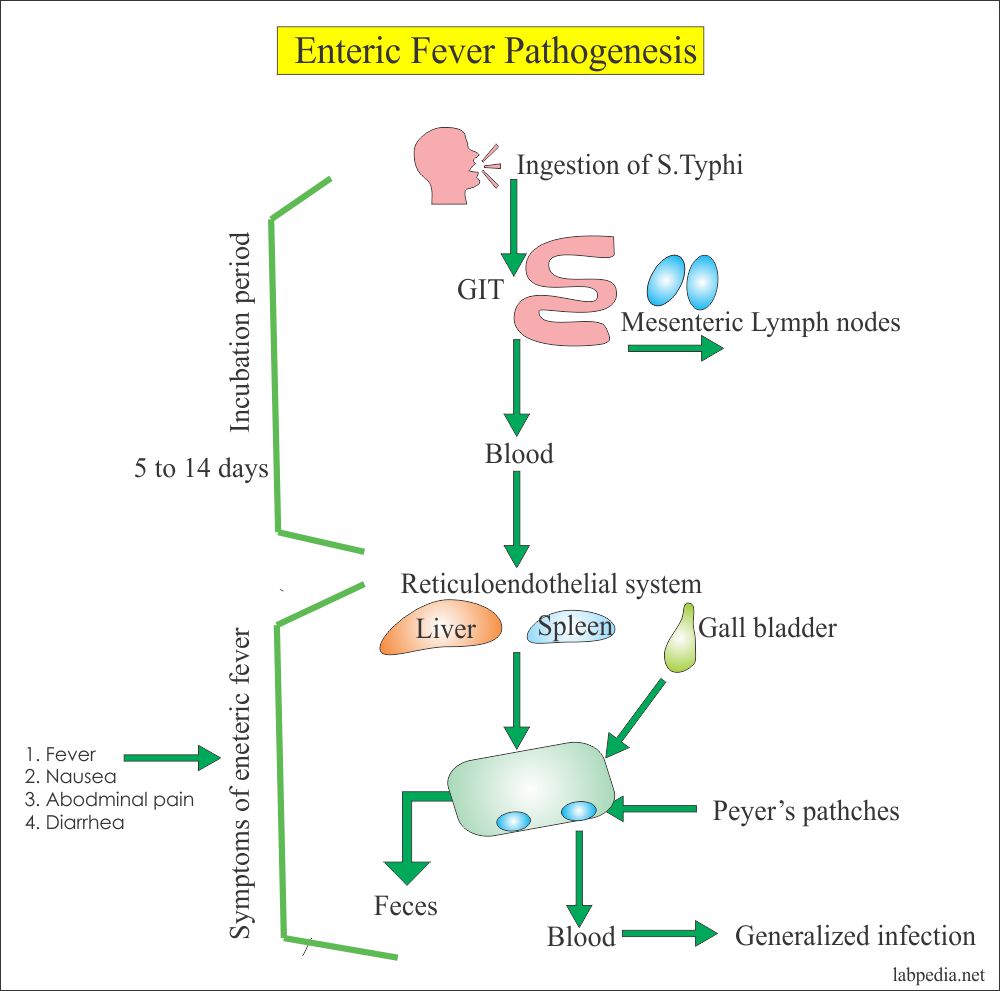
Enteric Fever
This is a bacterial infection characterized by abdominal tenderness, confusion, prolonged high fever, prostration and occasionally, a rash.
Causative organism; Salmonella typhi or Salmonella paratyphi
Mode of transmission; ingestion of food or water contaminated with the faeces of an infected person.
Following a 5 to 21 day incubation period, typical signs include diffuse abdominal pain, headache, prolonged fever, anorexia, nausea, loss of appetite and constipation or sometimes diarrhea. Daytime drowsiness and nighttime insomnia are characteristic signs.
Possible complications include gastrointestinal haemorrhage and perforation, heart failure and encephalitis. Effective antibiotics are available and the prognosis in patients under treatment is usually favorable.
 |
| Photo by labpedia.net |
Pathophysiology
Diarrhea is produce by increased intestinal secretions, decreased mucosal absorption, and altered motility. Diarrhea could be described as;
- Osmotic.
- Secretive.
- Mixed.
Osmotic diarrhea
Absorption of water in the intestines is dependent on adequate absorption of solutes. If excessive amounts of solutes are retained in the intestinal lumen, water will not be absorbed and diarrhea will result.
It may also occurs when water is pulled into the intestines by the osmotic pressure of unabsorbed particles but often results from malabsorption or the ingestion of a poorly absorbable Substrate. This type of diarrhea stops when patients are fasted or the consumption of the poorly absorbable substrate is ceased.
Secretory diarrhea
Large volumes of water are normally secreted into the small intestinal lumen, but a large proportion of this water is efficiently absorbed within the colon.
Diarrhea therefore occurs when secretion of water into the intestinal lumen exceeds absorption by the colon. It is often high volume diarrhea and may lead to severe dehydration.
Mixed diarrhea
Mixed diarrhea is caused by increased peristalsis (increased gastric motility) and combination of increase secretion and decreased absorption in the bowel.
Clinical manifestations
- Increased frequency and fluid content of stools.
- Abdominal cramps, tenderness and distention (bloating).
- Painful spasmodic contraction of the anus and ineffectual straining (i.e. tenesmus) may occur with defecation.
- Flatulence.
- There may be fever and diaphoresis (sweating, esp. to an unusual degree).
- Weakness or fatigue.
- Anorexia.
- Nausea.
- Intestinal rumbling (borborygmus).
- Perianal erythema or reddening.
- Severe and prolonged diarrhea results in fluid and electrolyte imbalances.
- Depressed consciousness.
- Sunken eyes and anterior fontanel.
- Dry mucous membranes.
- Increased thirst.
- Luck of tears.
- Poor skin turgor.
- Delayed capillary refill.
- Collapse of the veins especially of the neck veins.
- Scanty urine production and concentration (0.5 - 1ml/kg/hr of an adult and 1ml/kg/hr for a child).
- Restless or irritability.
- Hypovolemic shock.
- Deep/rapid and weak pulse.
- Low or absent Blood Pressure.
- Gold and clammy (moist) extremities.
- Altered consciousness.
- Malnutrition.
- Reduced muscle and fat mass or peripheral edema may be clues to the presence of carbohydrate, fat, and/ protein malabsorption.
Complication
- Dehydration.
- Damage to the intestinal mucosa.
- Renal failure.
- Sepsis.
- Malnutrition including vitamin and mineral deficiencies.
Diagnosis
- History and physical examination.
- Stool routine examination.
- Stool culture and sensitivity testing.
- Full blood count.
- Endoscopy.
- Barium enema.
Medical management
Management depends on severity and the underlying cause. In some cases, bed rest and increased oral fluid intake will suffice without the use of any drug.
- Diarrhea associated with high volume fluid loss will require aggressive oral or parenteral rehydration to correct dehydration and to prevent complications.
- Antibiotics (depends on the causative agent and should be used judiciously).
- Zinc supplementation o Antidiarrheal/anti-motility agents.
- Antipyretics.
Nursing management
- Isolate and adhere on infection prevention and control protocols.
- Encourage bed rest.
- Encourage the intake of liquids as much as patient can tolerate and foods low in bulk until diarrhea subsides.
- Keep an accurate intake and output chart and balance it every 24hrs.
- Recommend a bland diet of semisolid and solid foods.
- Discourage the intake of foods that stimulate the gastrointestinal tract including caffeine alcohol, carbonated beverages, milk and food that are very cold or hot.
- Maintain a calm demeanor when serving or removing bedpans or helping patient to tidy up. Care for the perianal area; wash area with soap, dry and apply barrier cream or talcum powder.
- Change patient clothing and bed linen as often as required to keep the perianal area dry and fresh.
- Manage other Symptoms as required e.g. fever, abdominal cramps etc.
Prevention and control
- Giving only breast milk for the first 6 months of life.
- Avoiding the use of infants feeding bottle.
- Improve practices related to the preparation and storage of weaning fluids and feeds.
- Wash hands with soap under running water after defecation or handling faeces, and before preparing food or eating.
Read Also






1 Comments
I'd like to express my gratitude for writing such an informative piece on this blog. This article provided me with a variety of data. Continue to post. abdominal pain emergency
ReplyDelete