Unlike most other bones, the bones comprising the vault of the foetal skull are formed from membrane and not from cartilage. In this membrane are five (5) points called ossification centres. The first signs of early skull development occur at the end of 4week of intrauterine life and commence in the occiput. As pregnancy advances, calcium is laid down around these centres and so the skull bone begins to develop calcification begins as early as the 5th weeks following conception. The chief function of skull is to protect the brain which lies within it. When a premature infant is born, the bones are still far from being completely ossified. Incomplete ossification is advantageous because it allows the skull bones to overlap slightly when the head is compressed and pushed through the pelvis by uterine contractions. The head is the leading part in about 95% of all labours and in relation to other parts of the foetus. For descriptive purposes the foetal skull is divided into three (3) regions.
1. The vault: the area above an imaginary line drawn below the occipital protuberance to the orbital ridges.
2. The face: the area extending from the orbital ridges to the junction of the chin and neck. It composed of 14 bones which are united.
3. The base: the
bones in this area also firmly united and help to protect the brain.
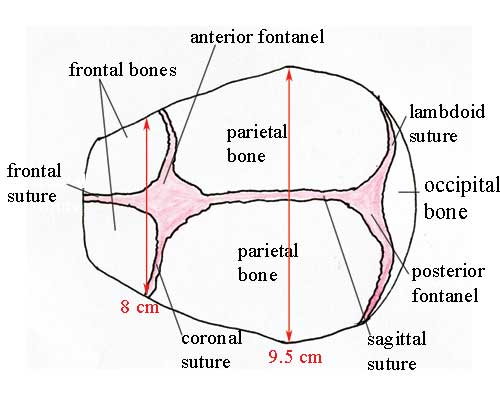
THE VAULT OF THE SKULL
 |
| Photo by open.edu |
THE BONESTHE OCCIPUT: one bone which lies Posterior. The ossification centre can be easily defined and is named the occipital protuberance.
THE PARIETAL: lateral on the right and left are the parietal bones with their ossification centres, the parietal eminence.
THE FRONTAL: anteriorly lies the right and left frontal bones, whose ossification centre are named frontal eminences or frontal bosses.
SUTURES: is an area of membrane between the skull bones where ossification has not been completed.
LAMBDOIDAL SUTURE: lies between the occiput and the parietal bones.
SAGITTAL SUTURE: this divides the parietal bones.
CORONAL SUTURE: it separates the parietal bone from the frontal bones.
FRONTAL SUTURE: it divides the frontal bones.
THE POSTERIOR FONTANELLE: This occurs at the junction of the lambdoidal and sagittal sutures. It is very small and triangular in shape and does not close until the infant is 6 week old.
THE ANTERIOR FONTANELLE: This is formed where the sagittal, coronal and frontal sutures meet and it is diamond shaped. It is much larger than the posterior fontanelle being approximately 2.5cm in length and 1.3cm wide. The anterior fontanelle should be completely ossified by the time that the infant is 18 month of age
AREAS OF THE SKULL
GLABELLA: the bridge of the nose
SINCIPUT: the forehead.
BREGMA: the anterior fontanelle.
VERTEX: the highest point on the foetal skull. It lies on the sagittal suture midway between the parietal eminences. The term vertex is use to describe an area bounded by the anterior and posterior fontanelle and the parietal eminence.
LAMBDA: the posterior fontanelle.
OCCIPUT: the area occupied by that bone
THE MENTUM: the chin
SUDOCCIPITAL AREA: lies below the occipital protuberance
MEASURMENT OF THE FOETAL SKULL: This depends on the attitude of the foetal head and the measurement which must enters the birth canal.
ATTITUDE: this is the relationship of the foetal head and limbs to its trunk. It varies from flexion and full extension.
THE ENGAGING DIAMETER: this is the diameter of the fetal head that enters the pelvis and it also depends on the attitude of the foetus.
THE COMMON DIAMETER OF THE FOETAL SKULL
Sub-occipito bregmatic diameter is 9.5cm.
The occipito-frontal diameter is 11.5cm.
The sub-occipito-frontal diameter is 10cm.
Sub-mento bregmatic diameter is 9.5cm.
Submento vertical diameter is 11cm.
Mentovertical diameter is 13.5cm.
The biparietal diameter is 9.5cm.
The bi-temporal
diameter is 8.2cm.
THE CIRCUMFERENCE OF THE FOETAL SKULL
1. The sub-occipito bregmatic circumference is measured 30-33cm.
2. The occipito frontal circumferences measured 25cm.
3. The mento-vertical circumferences measured 38cm.
MOULDING
is the alteration in shape of the foetal skull to enable it pass through the birth canal.
FACTORS THAT ASSIST IN MOULDING
1 The uterine action pushes down the head to the birth canal
2 Counter pressure of the pelvic organs from the below and bony pelvis.
3 The suture and fontanelle help bones to overlap each other
METHODS OF MOULDING
1. The frontal and occipital bones slides under the parietal.
2. The posterior parietal bones pass under the anterior parietal bone.
TYPES OF MOULDING
Excessive moulding or abnormal
this occurs when labour is prolonged, due to disproportion between the size of the foetal head and the maternal pelvis or when the skull bones are not completely ossified and therefore offer little resistance to pressure.
Upward moulding/sugar loaf moulding
when the occipito frontal diameter is the engaging diameter. Moulding occurs in the submento bregmatic direction, so that the falx cerebri is pull upwards. It is likely to tear at is junction with the tentorium and rupture of the membranes in this area will also involve large blood vessels, resulting intracranial haemorrhage.
Rapid moulding
rapid compression and decompression of the head is the commonest cause of rupture of the cerebral membranes. Any infant who has been subject to severe moulding will suffer some degree of asphyxia at birth as a result of intracranial compression. Any such infant who show signs of cerebral irritation, should be seen immediately by a pediatrician, who will most likely prescribe I.M Vitamin K 0.5-1 mg depending upon the infant’s weight and condition.
Normal moulding
the engaging diameter is reduced of which the diameter which runs at right angle is elongated in the same proportion and this depends on the attitude of the foetal head. In vertex presentation, the sub-occipito bregmatic diameter is reduced and mento-vertical diameter is elongated and lengthened. Moulding disappears after 24 hours. If moulding is moderate, it is beneficial, but if excessive, intracranial haemorrhage can result.
CEREBRAL MEMBRANES
The brain and the spinal cord are covered by membrane called meninges. There are 3 coverings; Duramater, arachinord mater and pia mater.
Dura mater: is the most important to the nurse as it lies superficially. It is a strong fibrous membrane consisting of two (2) layers. The outer layer is attached to the bones and the inner layer covers the outer surface of the brain with 2 important folds namely:
- The falx cerebri: is a sickle shaped cell membrane separating 2 cerebral lobes at the cerebrum starting from the root of the nose following the frontal and sagittal suture is attach to the occipital bones.
- The tentorium cerebellum: is the tent like in shape lying in horizontal position, which separates the cerebrum and the cerebellum. They contain the sinuses joined by the falx cerebri. Posteriorly and longitudinally sinuses joined by the straight sinus (the great vein of Galen).If moulding is excessive, the membranes may tear involving the tentorium and great vein of Galen to cause intracranial haemorrhage which may cause the death of the foetus or affect its health
Two (2) conditions which arise during labour and both cause a swelling on the infant’s head.1. Caput succedaneum: is an edematous swelling of the subcutaneous tissues of the foetal skull. It occurs following early rupture of membrane in the first stage of labour because there is no bag of fore waters to take the pressure of the dilating cervix off the foetal head.
CHARACTERISTICS OF CAPUT SUCCEDANEUM
1 It present at birth
2 It may lie over a suture line
3 Because it is edematous, it puts on pressure.
4 It disappears completely within 24-48 hours
No treatment is requires unless the caput is of excessive size. But observe for sign of cerebral irritation.
2. Cephalhaematoma: this is swelling due to bleeding between the skull bone and the periosteum as overriding of the bones take place during moulding. A low prothrombin level is probably a factor.
CHARACTERISTIC OF CEPHALHAEMATOMA
1 It is not present at birth but appear 2-3 days afterward.
2 It occurs over a bone area, although it may be bilateral.
3 The head is usually more red and bruised in appearance than caput succedaneum.
4 The swelling may increase and it takes 6 weeks at least to disappear completely.







1 Comments
I am glad that I came here and I can gain more information about this. You have written this article very factual which is understandable for everyone, Thanks for share it. 4d Ultrasound Perth
ReplyDelete